
 |
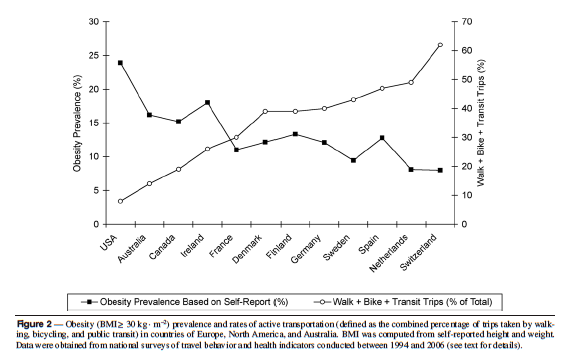
| Graph (above, Figure 2) from: Bassett, Jr., et al.,
Walking, cycling, and obesity rates in Europe, North America, and Australia, Journal of Physical Activity and Health, 5, 795-814
|
Bicycles have been around for a long time. There is a sketch for an early bicycle design in one of Leonardo da Vinci’s pupils’ notebooks from 1493. Over the years bicycles have been upgraded and modified, moving from being a luxury of the wealthy to the transportation of the masses. The advent of cars slowed bicycle usage in industrialized countries, but in less economically developed countries bicycles are still a primary mode of transporting people and goods. Likewise the production of bicycles has remained nearly double that of cars.
For many countries bicycles are at the front lines of public health, they just may not realize it. The US has been watching a steady rise in obesity rates as a result of inactivity and unhealthy diet choices. Many states and cities are working to implement programs to increase bike usage including: Rails to Trails projects, Bike sharing in Washington DC and Nashville, as well as increased bike lanes linking residential areas to commercial zones. These programs will all have a big impact of the health of the US population. The CDC states that the number on strategy for increasing physical activity is shifting from car trips to walking or biking. Bicycling Magazine notes that new bicycle commuters can expect to lose up to 13 pounds their first year of biking to work.
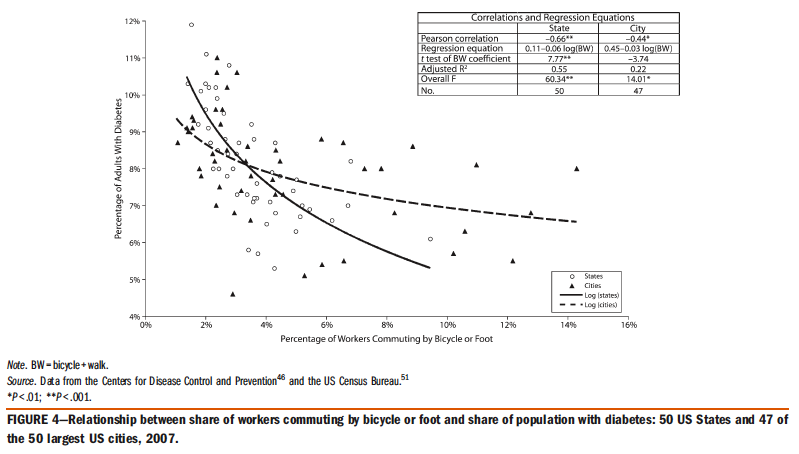 |
| Graph (above, Figure 4) from: Pucher, J., et al., 2010
Walking and cycling to health: A comparative analysis of city, state, and international data, American Journal of Public Health, published online ahead of print
|
The benefits are huge, but that doesn’t always make it easy for people to jump right on a bike. A recent study led by Dr. John Pucher of Rutgers University found a direct correlation between percentages of adults with diabetes and percentages of commuters biking or walking to work in 47 of the 50 largest US cities (Walking and Cycling for Health, August 2010). To state the obvious, the increase in programs that promote bike usage and the increase in people biking will have a very positive effect on the health of populations
However, the US isn’t the only country working to get its citizens moving. Copenhagen (Denmark), known for being a biking city, launched “You won’t believe it… You’re safer on the bicycle than on the sofa!” A campaign run by the city’s Public Health office, their goal was to get more people biking to work instead of taking their car for a short trip. The campaign told Copenhagen residents, “Lack of movement in everyday life is harmful to health, while physical activity keeps the body healthy. Daily exercise for at least 30 minutes prolongs life by up to 5 years, and cycling can thus help to prolong life.” Even as a strong biking city even Copenhagen felt the need to better educate and mobilize its population. As can easily be guessed Denmark has a low rate of obesity at 9.5%.
In “developing” countries of the world obesity rates aren’t the greatest health risk, nor is low physical activity often a common unhealthy lifestyle. The health risks in “developing” countries are often related to access to health services and emergency transportation. Surely this isn’t an area where bicycles can have an impact!
In many low resource setting around the world, Community Health Workers (CHWs) travel from village to village, home to home to deliver health education and services. In many places CHWs rely on bicycles as their only means of getting from one place to another. Bikes Without Borders highlights the work of CHWs in Malawi utilizing bikes to increase their effectiveness and to help more people. Bicycles for Humanity collects almost 50,000 bikes a year and sends them to organizations that distribute them most often to healthcare workers and women. Since women do a majority of traveling in “developing” countries, a bike can help them to transport themselves, water containers, and goods to market.
Bicycles have even been modified to serve as ambulances in areas where there is no emergency transportation. The Bicycle Empowerment Network (BEN) in Namibia has implemented a very effective model for faster transportation where there is none. Drivers of the bicycle ambulances come from local organization and they receive training on use and maintenance.
Whether it is in the post-industrial cities of the US, modern cities of Europe, or in some of the world’s poorest regions, the simplest transportation technology can have huge impacts on the future health of our population.
Featured on the Americans for Informed Democracy Blog, where I’m blogging as a Global Health Analyst.





